Short-term memory has several key characteristics and limitations, especially when it comes to interruptions:
1. Limited capacity: Short-term memory can typically hold only about 7 (+/- 2) items at a time. This limited capacity makes it vulnerable to disruption when new information is introduced.
2. Short duration: Information in short-term memory typically lasts only about 20-30 seconds unless it is actively rehearsed or transferred to long-term memory. Interruptions can easily disrupt this process.
3. Susceptibility to interference: Short-term memory is highly susceptible to interference from similar information or distractions. When interrupted, the contents of short-term memory can be quickly displaced or forgotten.
4. Attention-dependent: Maintaining information in short-term memory requires active attention. Interruptions divert attention away from the information being held, leading to rapid forgetting.
5. Fragility of encoding: The process of encoding information into short-term memory is easily disrupted. Interruptions during this critical phase can prevent proper encoding altogether.
6. Rehearsal disruption: People often use mental rehearsal to keep information in short-term memory. Interruptions break this rehearsal process, causing rapid decay of the held information.
7. Context-dependent recall: Short-term memory retrieval often relies on the mental context present during encoding. Interruptions can change this context, making it harder to recall the original information.
8. Limited processing: Short-term memory has limited processing capabilities. Complex interruptions can overwhelm these resources, leading to information loss.
9. Vulnerability to stress: Interruptions can induce stress, which further impairs short-term memory function and capacity.
10. Serial position effect: Items at the beginning and end of a sequence are often better remembered than those in the middle. Interruptions can disrupt this effect, particularly for more recently presented items.
11. Modality-specific interference: Interruptions in the same modality (e.g., auditory interruptions for auditory information) tend to be more disruptive than cross-modal interruptions.
12. Task-switching costs: Switching between tasks (as caused by interruptions) incurs cognitive costs, reducing the efficiency of short-term memory operations.
To mitigate these weaknesses, strategies like chunking information, immediate rehearsal, and minimizing distractions can be employed. Additionally, quickly writing down important information or using mnemonic devices can help preserve it in the face of potential interruptions.

Trading psychology is a critical aspect of successful investing that often goes overlooked by novice traders. Understanding the psychological factors that influence trading decisions can be the difference between consistent profits and devastating losses. In this comprehensive guide, we'll explore the intricacies of trading psychology, its impact on financial markets, and strategies to improve your mental approach to trading.
What Is Trading Psychology?
Trading psychology refers to the emotional and mental state of a trader that influences their decision-making process in financial markets. It encompasses a wide range of psychological factors, including emotions, cognitive biases, and behavioral patterns that can affect trading performance[1].
The stock market is not just a collection of numbers and charts; it's a reflection of human psychology in action. Every buy or sell order represents a decision made by an individual or institution, often influenced by complex psychological factors. Understanding these factors can provide traders with a significant edge in the market.
The Importance of Trading Psychology
Mastering trading psychology is crucial for several reasons:
1. Emotional Control: The ability to manage emotions like fear, greed, and anxiety is essential for making rational trading decisions.
2. Discipline: A strong psychological foundation helps traders stick to their trading plans and avoid impulsive actions.
3. Risk Management: Understanding one's psychological tendencies can lead to better risk assessment and management.
4. Consistency: A stable psychological state contributes to more consistent trading performance over time.
5. Resilience: The mental fortitude developed through good trading psychology helps traders bounce back from losses and setbacks.
The Role of Trading Psychology in Successful Trading
Successful trading is not just about having the right strategy or technical skills; it's equally about having the right mindset. Trading psychology plays a pivotal role in determining a trader's success by influencing how decisions are made under conditions of uncertainty and risk[1].
Benefits of Adopting a Trading Psychology Mindset
1. Improved Decision-Making: A strong psychological foundation leads to more rational and objective decision-making.
2. Better Stress Management: Understanding one's psychological triggers helps in managing stress during volatile market conditions.
3. Enhanced Discipline: A proper trading psychology mindset reinforces the importance of following a trading plan.
4. Increased Confidence: As traders become more aware of their psychological patterns, they often gain confidence in their abilities.
5. Long-Term Perspective: A good trading psychology helps maintain focus on long-term goals rather than short-term fluctuations.
Common Psychological Mistakes in Trading
1. Overconfidence: Believing one can consistently beat the market without proper analysis or risk management.
2. Fear of Missing Out (FOMO): Making impulsive trades based on the fear of missing potential profits.
3. Anchoring: Fixating on a specific price point or past performance, ignoring new information.
4. Confirmation Bias: Seeking out information that confirms pre-existing beliefs while ignoring contradictory evidence.
5. Loss Aversion: Holding onto losing positions too long in hopes of breaking even.
What Is Behavioral Finance?
Behavioral finance is a field that combines psychological theory with conventional economics and finance to provide explanations for why people make irrational financial decisions. It challenges the traditional assumption that markets and investors are perfectly rational[1].
Key Concepts in Behavioral Finance
1. Prospect Theory: People value gains and losses differently, often showing a stronger aversion to losses than attraction to equivalent gains.
2. Mental Accounting: The tendency to categorize and evaluate economic outcomes by grouping them into separate accounts.
3. Herd Behavior: The propensity for individuals to mimic the actions of a larger group, often leading to market bubbles or crashes.
4. Overreaction and Underreaction: Investors tend to overreact to unexpected news events and underreact to new information about a stock.
5. Cognitive Dissonance: The mental discomfort experienced when holding conflicting beliefs, often leading to irrational justifications for trading decisions.
Behavioral Biases in Investing
Behavioral biases are systematic errors in judgment that can lead to irrational decision-making in trading and investing. Recognizing these biases is crucial for developing a strong trading psychology.
Common Behavioral Biases
1. Confirmation Bias: The tendency to search for or interpret information in a way that confirms pre-existing beliefs.
2. Availability Bias: Making decisions based on information that is readily available rather than all relevant information.
3. Recency Bias: Giving more importance to recent events and overlooking historical patterns.
4. Sunk Cost Fallacy: Continuing to invest in a losing position because of the resources already committed.
5. Gambler's Fallacy: Believing that past events can influence future outcomes in random processes.
Different Types of Emotional Biases in Trading
Emotional biases are deeply ingrained and often more challenging to overcome than cognitive biases. These biases can significantly impact trading decisions and overall performance[1].
Fear and Greed
Fear and greed are perhaps the two most powerful emotions in trading. Fear can lead to:
- Exiting profitable trades too early
- Hesitating to enter trades despite clear signals
- Overtrading in an attempt to recover losses
Greed, on the other hand, can result in:
- Holding winning positions too long
- Taking on excessive risk
- Ignoring warning signs in the market
Overconfidence and Complacency
Overconfidence often stems from a string of successful trades, leading traders to:
- Underestimate market risks
- Overtrade or increase position sizes beyond their risk tolerance
- Ignore contradictory information
Complacency can set in when markets are calm, causing traders to:
- Neglect proper risk management
- Fail to adapt to changing market conditions
- Become less vigilant in their analysis
Impatience and Impulsivity
The fast-paced nature of trading can breed impatience and impulsivity, leading to:
- Entering trades without proper analysis
- Exiting positions prematurely
- Overtrading in an attempt to force profits
Loss Aversion
Loss aversion, the tendency to prefer avoiding losses over acquiring equivalent gains, can cause traders to:
- Hold onto losing positions too long
- Take profits too quickly on winning trades
- Avoid taking necessary risks
Anchoring Bias
Anchoring occurs when traders rely too heavily on a single piece of information when making decisions. This can lead to:
- Fixating on a stock's past price, ignoring fundamental changes
- Stubbornly maintaining a price target despite new information
- Basing future expectations on past performance
How Bias Affects Trading
Biases can have a profound impact on trading performance, often leading to suboptimal decisions and missed opportunities.
Negativity Bias
Negativity bias, the tendency to give more weight to negative experiences, can result in:
- Overemphasizing potential losses
- Hesitating to enter trades after experiencing losses
- Developing an overly pessimistic market outlook
Gambler's Fallacy
The gambler's fallacy can lead traders to:
- Believe that a losing streak must end soon, leading to increased risk-taking
- Assume that a winning streak will continue indefinitely
- Make decisions based on patterns in random events
Status Quo Bias
Status quo bias, the preference for the current state of affairs, can cause traders to:
- Resist adapting to changing market conditions
- Hold onto positions longer than they should
- Avoid exploring new trading strategies or instruments
Strategies to Combat Emotional Bias in Trading
Developing strategies to combat emotional biases is essential for improving trading psychology and overall performance.
Recognizing Emotions During Trades
1. Practice Mindfulness: Develop awareness of your emotional state while trading.
2. Use Emotion Tracking Tools: Implement software or apps that help monitor your emotional responses.
3. Establish Emotional Checkpoints: Regularly assess your emotional state at key decision points.
Journaling to Track Your Thoughts & Feelings
1. Maintain a Detailed Trading Journal: Record not just trades but also thoughts and emotions.
2. Analyze Patterns: Look for correlations between emotional states and trading outcomes.
3. Reflect Regularly: Set aside time to review your journal and identify areas for improvement.
Having a Solid Trading Plan
1. Develop Clear Entry and Exit Criteria: Establish specific rules for when to enter and exit trades.
2. Set Realistic Profit Targets and Stop-Losses: Define risk-reward ratios for each trade.
3. Create a Pre-Trade Checklist: Use a systematic approach to evaluate potential trades.
Understanding Their Risk Appetite
1. Assess Your Risk Tolerance: Be honest about how much risk you can comfortably handle.
2. Align Trading Strategy with Risk Tolerance: Choose strategies that match your risk profile.
3. Regularly Re-evaluate Risk Levels: As circumstances change, adjust your risk management approach.
Knowing When to Take a Break
1. Set Trading Time Limits: Establish specific hours for trading to avoid burnout.
2. Recognize Emotional Fatigue: Learn to identify when emotions are clouding judgment.
3. Implement Mandatory Rest Periods: Schedule regular breaks, especially after intense trading sessions.
Honing Your Mindset
1. Continuous Education: Stay informed about market trends and trading psychology.
2. Practice Visualization: Mentally rehearse calm and rational responses to various market scenarios.
3. Develop a Growth Mindset: View challenges and losses as opportunities for learning and improvement.
How to Improve Your Trading Psychology
1. Educate Yourself: Read
trading books, attend seminars, and study successful traders to gain insights into effective trading psychology.
2. Practice with Paper Trading: Use simulated trading to experiment with different strategies without financial risk.
3. Seek Mentorship: Learn from experienced traders who can provide guidance on psychological aspects of trading.
4. Develop a Routine: Establish a consistent pre-trading routine to prepare mentally for the day ahead.
5. Set Realistic Goals: Create achievable short-term and long-term trading objectives.
6. Practice Stress Management: Incorporate stress-reduction techniques like meditation or exercise into your daily routine.
7. Learn from Mistakes: Analyze losing trades objectively to identify psychological factors that may have contributed.
8. Celebrate Successes: Acknowledge and reward yourself for following your trading plan, regardless of outcomes.
9. Stay Physically Healthy: Maintain a balanced diet, regular exercise, and adequate sleep to support mental clarity.
10. Join a Trading Community: Engage with other traders to share experiences and learn from collective wisdom.
Conclusion
Trading psychology is a fundamental aspect of successful trading that often separates profitable traders from those who struggle. By understanding the various psychological factors that influence trading decisions, recognizing common biases, and implementing strategies to combat emotional reactions, traders can significantly improve their performance and consistency.
Remember that developing strong trading psychology is an ongoing process. It requires continuous self-reflection, learning, and practice. As you progress in your trading journey, always be mindful of the psychological aspects of your decision-making. With time and effort, you can cultivate a mindset that leads to more rational, disciplined, and ultimately successful trading.
By focusing on improving your trading psychology alongside your technical skills and market knowledge, you'll be better equipped to navigate the complex and often unpredictable world of financial markets. Stay committed to your psychological development, and you'll likely find that it becomes one of your most valuable assets as a trader.
Stock trading is a complex activity that challenges our cognitive abilities and emotional control. Despite the potential for significant financial gains, many individuals struggle to succeed in this arena. The reasons for these difficulties are deeply rooted in our evolutionary history and the psychological biases that have developed over millennia. Understanding these factors can help traders recognize their inherent limitations and develop strategies to overcome them.
Evolutionary Factors
Our brains evolved in an environment vastly different from today's financial markets. The traits that helped our ancestors survive in the wild can often work against us when making investment decisions. Let's explore some of these evolutionary factors in detail in
trading psychology to help you become a better trader.
Fear and Loss Aversion
One of the most powerful evolutionary traits that impact trading behavior is fear, particularly the fear of loss. Our brains are wired to prioritize avoiding losses over acquiring gains, a characteristic known as loss aversion. This trait served our ancestors well in survival situations, where the loss of resources or taking unnecessary risks could lead to death.
In the context of stock trading, loss aversion manifests in several ways:
1. Holding onto losing positions: Traders often refuse to sell stocks that have decreased in value, hoping they will recover. This behavior can lead to even greater losses as declining stocks continue to fall.
2. Selling winning positions too early: Conversely, traders may be quick to sell stocks that have increased in value, fearing that the gains might be lost if they hold on longer. This can result in missed opportunities for further growth.
3. Hesitation in entering new positions: The fear of potential losses can prevent traders from entering promising positions, leading to missed opportunities.
4. Overreaction to short-term market fluctuations: Loss aversion can cause traders to panic during market downturns, leading to impulsive selling decisions that may not align with long-term investment strategies.
The impact of loss aversion on trading decisions can be significant. Studies have shown that the pain of losing money is psychologically about twice as powerful as the pleasure of gaining the same amount. This imbalance can lead traders to make irrational decisions, prioritizing the avoidance of losses over the pursuit of gains, even when the latter may be more beneficial in the long run.
Greed and Reward-Seeking Behavior
While fear plays a significant role in trading behavior, greed is equally influential. The human brain releases dopamine, a neurotransmitter associated with pleasure and reward, in anticipation of potential gains. This neurochemical response can create a cycle of addictive behavior in trading.
The impact of greed and reward-seeking behavior on trading includes:
1. Overtrading: The thrill of potential gains can lead traders to execute more trades than necessary, increasing transaction costs and potentially exposing themselves to greater risk.
2. Excessive risk-taking: In pursuit of larger profits, traders may take on positions that are too large relative to their account size or risk tolerance.
3. Chasing trends: The fear of missing out (FOMO) can drive traders to jump into popular stocks or market trends without proper analysis, often buying at peak prices.
4. Neglecting diversification: Greed can cause traders to concentrate their investments in a few high-potential stocks, ignoring the benefits of a diversified portfolio.
5. Margin trading: The desire for amplified gains may lead traders to use leverage excessively, potentially magnifying losses.
The reward-seeking behavior driven by dopamine release can create a gambling-like mentality in trading. Successful trades trigger a dopamine rush, reinforcing the behavior and encouraging traders to seek out similar experiences. This can lead to a cycle of increasingly risky behavior as traders chase the "high" of successful trades.
Psychological Factors
In addition to evolutionary traits, various psychological biases significantly impact trading decisions. These cognitive biases are systematic patterns of deviation from norm or rationality in judgment, which can lead to perceptual distortion, inaccurate judgment, illogical interpretation, or what is broadly called irrationality.
Confirmation Bias
Confirmation bias is the tendency to search for, interpret, favor, and recall information in a way that confirms or supports one's prior beliefs or values. In the context of stock trading, this bias can have several detrimental effects:
1. Selective information processing: Traders may focus on news and analysis that support their existing positions while ignoring or downplaying contradictory information.
2. Overconfidence in predictions: Confirmation bias can lead traders to be overly confident in their market predictions, as they tend to remember their successful forecasts more than their failures.
3. Resistance to changing strategies: Traders may stick to ineffective trading strategies because they focus on instances where the strategy worked, ignoring overall poor performance.
4. Echo chamber effect: Traders might surround themselves with like-minded individuals or information sources, reinforcing their existing beliefs and potentially missing out on valuable diverse perspectives.
5. Misinterpretation of random events: Confirmation bias can cause traders to see patterns or trends in random market movements, leading to misguided trading decisions.
To combat confirmation bias, traders should actively seek out information that challenges their beliefs, consider alternative viewpoints, and regularly review their trading decisions with a critical eye.
Sunk Cost Fallacy
The sunk cost fallacy is the tendency to continue investing time, money, or effort into something because of previously invested resources, even when it's no longer rational to do so. This psychological bias can be particularly damaging in stock trading:
1. Refusing to sell losing positions: Traders may hold onto losing stocks because they've already invested a significant amount of money, hoping to recoup their losses rather than cutting their losses and moving on.
2. Averaging down on losing positions: The sunk cost fallacy can lead traders to buy more shares of a declining stock in an attempt to lower their average purchase price, potentially amplifying losses. This is also called a 'moron trade' as the trader is putting more on to their losing position.
3. Overcommitment to failed strategies: Traders may continue using unsuccessful trading strategies because of the time and effort already invested in developing and implementing them.
4. Emotional attachment to investments: The more time and resources invested in researching and monitoring a stock, the harder it becomes to let go, even when the investment is no longer sound.
5. Ignoring opportunity costs: Focusing on sunk costs can prevent traders from recognizing better opportunities elsewhere in the market.
To overcome the sunk cost fallacy, traders should focus on future potential rather than past investments. Regular portfolio reviews and setting clear, unemotional criteria for holding or selling positions can help mitigate this bias.
Overconfidence
Overconfidence is a cognitive bias in which a person's subjective confidence in their judgments is reliably greater than their objective accuracy. In trading, overconfidence can manifest in several ways:
1. Overestimating trading skills: Traders, especially after a string of successful trades, may overestimate their ability to predict market movements and make profitable decisions.
2. Underestimating risks: Overconfident traders often underestimate the risks associated with their trades, leading to inadequate risk management.
3. Ignoring market complexity: Overconfidence can cause traders to oversimplify complex market dynamics, leading to overly simplistic trading strategies.
4. Excessive trading: Overconfident traders may trade more frequently, believing they can consistently outperform the market, leading to higher transaction costs and potentially lower returns.
5. Neglecting education and improvement: Traders who are overconfident in their abilities may be less likely to seek out additional education or improve their trading strategies.
To combat overconfidence, traders should maintain a humble attitude, regularly assess their performance objectively, and seek feedback from other experienced traders or mentors.
Gambler's Fallacy
The gambler's fallacy is the mistaken belief that if something happens more frequently than normal during a given period, it will happen less frequently in the future (or vice versa). For example if a roulette ball has landed on a black number 5 times in a row, the gamblers fallacy is that red is due when point in fact, the odds are the same on every spin regardless of the streaks. This fallacy can significantly impact trading decisions:
1. Misinterpreting losing streaks: Traders may believe that a string of losing trades must be followed by winning trades, leading to continued poor decision-making.
2. Overvaluing recent performance: The gambler's fallacy can cause traders to give too much weight to recent market performance, expecting trends to reverse without fundamental reasons.
3 Ignoring random walk theory: This fallacy contradicts the idea that stock prices follow a random walk, leading traders to see patterns where none exist.
4. Misusing technical analysis: Traders may misinterpret chart patterns, believing that certain formations must lead to specific outcomes based on past occurrences.
5. Irrational position sizing: The gambler's fallacy can lead to increasing position sizes after losses, believing that a win is "due," potentially leading to catastrophic losses.
To avoid falling prey to the gambler's fallacy, traders should understand the principles of probability and randomness in financial markets. Each trade should be evaluated on its own merits, independent of past outcomes.
Cognitive Dissonance
Cognitive dissonance occurs when a person holds contradictory beliefs, ideas, or values, or when a person's beliefs are contradicted by new information. In trading, this can lead to several issues:
1. Difficulty admitting mistakes: Traders may struggle to acknowledge when they've made a poor trading decision, as it conflicts with their self-image as a skilled trader.
2. Rationalizing losses: To reduce dissonance, traders might create elaborate justifications for why a losing trade wasn't their fault or why it doesn't reflect their trading ability.
3. Inconsistent trading behavior: Cognitive dissonance can lead to inconsistencies between a trader's stated strategy and their actual trading behavior.
4. Resistance to new information: Traders may dismiss or downplay new information that contradicts their existing beliefs about a stock or the market.
5. Emotional stress: The tension created by cognitive dissonance can lead to emotional stress, potentially impacting future trading decisions.
To address cognitive dissonance, traders should practice self-awareness and be willing to critically examine their beliefs and decisions. Keeping a detailed trading journal can help identify inconsistencies between beliefs and actions.
Herd Mentality
Herd mentality, or the tendency for individuals to mimic the actions of a larger group, can significantly impact trading behavior:
1. Following market trends: Traders may buy or sell stocks simply because others are doing so, without conducting their own analysis.
2. Amplifying market movements: Herd behavior can lead to exaggerated market movements, creating bubbles during bull markets and panic selling during bear markets.
3. Ignoring fundamental analysis: The pressure to conform to group behavior can override rational decision-making based on fundamental analysis.
4. FOMO-driven decisions: Fear of missing out can drive traders to join market trends late, often buying at peak prices or selling at market bottoms.
5. Overreliance on financial media: Herd mentality can be reinforced by financial news and social media, leading to reactive rather than proactive trading strategies.
To combat herd mentality, traders might consider developing and sticking to their own well-researched strategies, avoid making impulsive decisions based on market sentiment, and maintain a long-term perspective.
Overcoming Evolutionary and Psychological Challenges in Trading
Understanding these evolutionary and psychological factors is the first step in overcoming them. Here are some strategies traders can employ to mitigate their impact:
1. Develop a robust trading plan: Create a detailed plan that outlines entry and exit criteria, position sizing rules, and risk management strategies. Stick to this plan to avoid emotional decision-making.
2. Use stop-loss orders: Implement stop-loss orders to automatically limit potential losses and remove the emotional aspect of closing losing positions.
3. Practice emotional discipline: Recognize and manage emotions during trading. Techniques such as mindfulness meditation can help maintain emotional balance.
4. Educate yourself: Continuously learn about market dynamics, trading strategies, and psychological biases. The more knowledgeable you are, the better equipped you'll be to make rational decisions.
5. Keep a trading journal: Maintain a detailed record of all trades, including the rationale behind each decision. Regularly review this journal to identify patterns and areas for improvement.
6. Seek diverse perspectives: Engage with traders who have different strategies and viewpoints to challenge your own beliefs and avoid confirmation bias.
7. Use technology wisely: Leverage trading tools and algorithms to help remove emotion from trading decisions, but be cautious of over-relying on technology.
8. Practice risk management: Implement proper position sizing and portfolio diversification to manage risk effectively.
9. Set realistic expectations: Understand that consistent profits are the result of disciplined trading over time, not overnight success.
10. Take regular breaks: Step away from trading periodically to maintain perspective and avoid burnout.
By understanding the biological and
psychological factors that influence trading behavior and implementing strategies to counteract them, traders can work towards more rational, disciplined, and potentially more successful trading practices. However, it's important to remember that trading always involves risk, and past performance does not guarantee future results. Continuous learning, adaptation, and self-reflection are key to long-term success in the challenging world of stock trading.
In the ever-evolving world of wearable technology, the Oura Ring has emerged as a game-changer, particularly in the realm of sleep tracking. This sleek, unobtrusive device is redefining how we monitor our health and wellness, offering a level of insight that many traditional fitness trackers struggle to match. If you're considering investing in a health tracker that prioritizes sleep quality and overall well-being, the Oura Ring might just be the perfect fit for you.
The Oura Ring: A New Approach to Health Tracking
The Oura Ring stands out in the crowded fitness tracker market with its unique form factor. Unlike bulky smartwatches or wristbands, this device cleverly disguises itself as a stylish piece of jewelry. Available in two designs - Heritage and Horizon - and crafted from a blend of titanium and plastic, the Oura Ring caters to diverse style preferences while delivering powerful health insights.
Key Features That Set Oura Apart
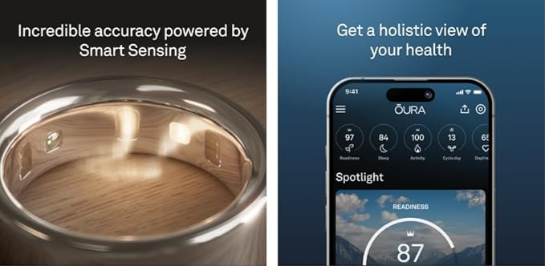
1. Comprehensive Sleep Analysis: The Oura Ring excels in sleep tracking, providing detailed insights into sleep patterns and trends that surpass many of its competitors.
2. Discreet Design: Its ring form factor offers a level of comfort and discretion that wrist-worn devices simply can't match, making it ideal for 24/7 wear.
3. Extended Battery Life: With up to 7 days of use on a single charge, the Oura Ring outperforms many smartwatches in terms of battery longevity.
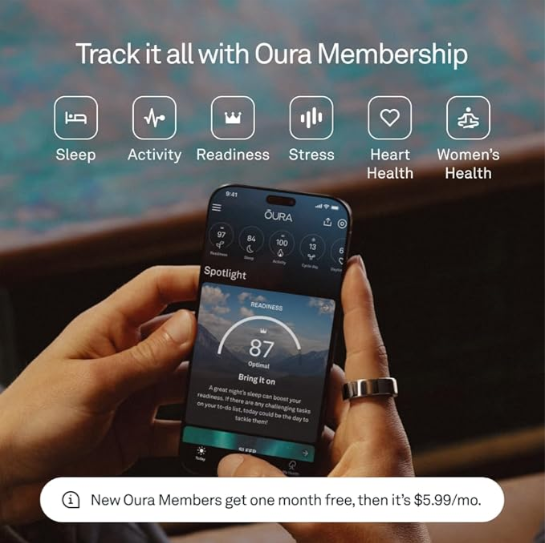
4. Holistic Health Monitoring: Beyond sleep, the ring tracks various metrics including heart rate, blood oxygen levels, skin temperature, and daily activity.
5. Unique Scoring System: Oura provides daily Readiness, Sleep, and Activity scores, offering an easy-to-understand overview of your overall health.
Revolutionary Sleep Tracking Capabilities
The Oura Ring's sleep tracking capabilities are where it truly shines, offering a level of detail and accuracy that sets it apart from other fitness trackers.
Comprehensive Sleep Metrics
The Oura Ring tracks a wide range of sleep-related metrics, including:
- Total sleep time
- Sleep efficiency
- Sleep latency (time taken to fall asleep)
- Sleep stages (light, deep, and REM sleep)
- Resting heart rate during sleep
- Heart rate variability (HRV)
- Respiratory rate
- Body temperature variations
This comprehensive data collection allows for a more nuanced understanding of your sleep quality than what most wrist-worn devices can provide.
Accuracy and Precision
The Oura Ring's sleep tracking accuracy has significantly improved over time. The third-generation ring has shown an impressive 79% agreement with polysomnography (the gold standard for sleep tracking), a substantial improvement from the 66% accuracy of the first generation[1]. This level of accuracy is particularly noteworthy in its ability to differentiate between sleep stages, outperforming many other wearables in this crucial aspect.
Sleep Score: A Holistic View of Your Rest
One of the Oura Ring's standout features is its daily Sleep Score. This easy-to-understand metric takes into account various aspects of your sleep, including total sleep time, efficiency, restfulness, REM sleep, and deep sleep. By providing a single, comprehensive score, Oura makes it simple for users to track their sleep quality over time and make informed decisions about their sleep habits.
Temperature Tracking: A Unique Advantage
Unlike many wrist-worn devices, the Oura Ring tracks body temperature changes during sleep. This feature not only helps in detecting potential illnesses but can also be valuable for women tracking their menstrual cycles or for those trying to conceive[3]. The ability to monitor temperature fluctuations adds another layer of insight into your overall health that many other trackers simply can't provide.
Beyond Sleep: A Holistic Approach to Health
While the Oura Ring excels in sleep tracking, its capabilities extend far beyond monitoring your nightly rest.
Activity Tracking
The Oura Ring automatically logs various physical activities, including running, cycling, and strength training. It provides an Activity Score that reflects your daily movement levels, encouraging you to maintain an active lifestyle. While it may not offer the real-time feedback that some dedicated fitness watches provide, its ability to seamlessly track your activity without the need for manual input is a significant advantage for many users.
Readiness Score: Your Daily Health Compass
One of the Oura Ring's most innovative features is its Readiness Score. This daily metric takes into account various factors including your sleep quality, activity levels, body temperature, and recovery status to give you an indication of how prepared your body is for the day ahead. This feature can be particularly valuable for athletes or anyone looking to optimize their training and recovery.
Stress and Recovery Monitoring
By tracking heart rate variability (HRV) and other physiological markers, the Oura Ring provides insights into your stress levels and recovery status. This information can be crucial for managing your overall well-being and avoiding burnout.
User Experience and App Integration
The Oura Ring's user-friendly app is a key component of its appeal. The app presents your data in an easily interpretable format, making it accessible even for those without a technical background[1]. It offers personalized insights and recommendations based on your data, helping you make informed decisions about your health and lifestyle.
Personalized Insights
After 90 days of use, Oura determines your chronotype and optimal sleep schedule, offering tailored advice to improve your sleep quality. This level of personalization sets Oura apart from many other health trackers, providing value that extends beyond mere data collection.
Integration with Other Health Apps
The Oura Ring integrates seamlessly with popular health and fitness apps. For instance, its partnership with Strava allows for automatic tracking of runs and cycling sessions, contributing to a more comprehensive view of your fitness activities.
Comfort and Practicality
One of the Oura Ring's biggest selling points is its comfort and practicality for 24/7 wear.
Designed for Continuous Use
The ring's lightweight titanium construction makes it comfortable to wear day and night. Unlike bulky smartwatches, you're less likely to feel the need to remove it during sleep or other activities.
Water-Resistant Design
The Oura Ring is water-resistant, allowing you to wear it during various activities, including swimming. This feature ensures uninterrupted tracking of your health metrics throughout the day.
Long Battery Life
With a battery life of up to 7 days, the Oura Ring requires less frequent charging compared to most smartwatches. This extended battery life contributes to its ability to provide continuous, uninterrupted health tracking.
Comparing Oura to Other Fitness Trackers
While the Oura Ring offers unique advantages, it's important to consider how it stacks up against other popular fitness trackers.
Oura vs. Apple Watch
Both devices track similar metrics, but the Oura Ring is often preferred for sleep tracking due to its comfort and more detailed sleep stage analysis. However, the Apple Watch offers features like real-time workout tracking and smartwatch functionalities that the Oura Ring doesn't provide.
Oura vs. Fitbit and Other Wearables
Compared to Fitbit and other wrist-worn trackers, the Oura Ring generally provides more comprehensive sleep data and is often considered more accurate, especially for sleep stage differentiation. However, it lacks the real-time display and extensive workout tracking features that some dedicated fitness trackers offer.
Potential Limitations
While the Oura Ring offers numerous advantages, it's important to consider its limitations:
1. No Real-Time Display: Unlike smartwatches, the Oura Ring lacks a screen for immediate data viewing. All information is accessed through the smartphone app.
2. Limited Active Workout Tracking: The ring doesn't provide real-time fitness statistics during workouts, which may be a drawback for some users.
3. Subscription Model: Full access to advanced sleep insights and other features requires a monthly subscription ($5.99/month or $69.99/year).

4. Size Limitations: The ring is only available in full sizes, which may affect the fit for some users.
Is the Oura Ring Right for You?
- Prioritize sleep quality and want detailed insights into their sleep patterns
- Prefer a discreet, comfortable health tracker that can be worn 24/7
- Are interested in a holistic view of their health, including stress levels and recovery
- Don't require real-time workout statistics or smartwatch functionalities
If you're primarily focused on active fitness tracking with real-time feedback during workouts, or if you prefer the additional features of a smartwatch, you might find other options more suitable.
Conclusion: A Revolutionary Approach to Health Tracking
The Oura Ring represents a significant leap forward in the world of health tracking, particularly in its approach to sleep monitoring. Its combination of advanced sensors, comfortable design, and comprehensive health insights make it a compelling choice for those looking to gain a deeper understanding of their overall well-being.
While it may not replace traditional smartwatches for everyone, the Oura Ring offers a unique and valuable perspective on your health that many other devices simply can't match. Its focus on sleep quality, recovery, and overall readiness provides a holistic view of your health that can lead to meaningful improvements in your daily life.
For those who prioritize sleep quality and are looking for a discreet, comfortable way to track their health metrics around the clock, the Oura Ring is an investment worth considering. Its ability to provide detailed, actionable insights into your sleep patterns, combined with its overall health tracking capabilities, makes it a powerful tool for anyone looking to optimize their well-being.
In a world where our health data is increasingly valuable, the Oura Ring stands out as a sophisticated, user-friendly device that can help you make informed decisions about your lifestyle. Whether you're an athlete looking to optimize your performance, a busy professional trying to balance work and wellness, or simply someone who wants to improve their sleep quality, the Oura Ring offers a unique and powerful solution.
By choosing the Oura Ring, you're not just buying a fitness tracker; you're investing in a comprehensive health monitoring system that can provide valuable insights for years to come. With its continuous improvements and updates, the Oura Ring is poised to remain at the forefront of personal health technology, making it a wise choice for those serious about understanding and improving their overall well-being.