Having traumatic memories can last for years, but fortunately some are able to be erasing PTSD with a natural mechanism in the brain fro rewriting memories. This process is known as memory reconsolidation and in this post is a review of a case study where a Vietnam veteran with 4 horrific PTSD memories has them erased and their significant units of distress (SUD's) reduced to zero.
- Introduction: High PTSD chronicity rates among military personnel necessitate novel treatments. Current frontline treatments (Prolonged Exposure, Cognitive Processing Therapy) show limited success and high dropout rates.
- The Reconsolidation of Traumatic Memories (RTM) Protocol: A brief, non-traumatizing intervention (fewer than 5 hours) utilizing the reconsolidation model of memory modification. It doesn't require full trauma re-exposure.
- Mechanism: Briefly activating the traumatic memory renders it susceptible to change. The intervention alters the memory's perceptual structure (third-person perspective, loss of colour, distance, granularity), reducing emotional intensity.
- Process:
- Client briefly recounts trauma; narrative terminated upon autonomic arousal.
- Reorientation to the present.
- SUDs (Subjective Units of Distress) ratings obtained.
- "Bookends" identified (pre- and post-trauma safe points).
- Imaginal movie theatre created; black and white movie of the trauma viewed dissociatively.
- Associated, reversed movie viewed, "undoing" the trauma from the safe post-trauma point.
- Probing for previous triggers; SUDs ratings.
- Creation and practice of alternate, non-traumatizing scenarios.
- Final trauma narrative recounting; SUDs ratings. The process is structured yet highly individualized.
- Therapist intervention to prevent re-traumatization via reorientation techniques if autonomic arousal is observed.
- RTM vs. Traditional TFCBT: While technically a Trauma-Focused Cognitive Behavioural Therapy (TFCBT), RTM differs significantly. The brief, non-reinforced exposure avoids extinction processes and prevents re-traumatization. Reconsolidation, not extinction, is the targeted mechanism.
- Case Study: Carl (Vietnam Veteran): A 46-year PTSD sufferer participating in a 30-person RCT of RTM. He had high pre-treatment PCL-M (73) and PSS-I (42) scores, experiencing frequent flashbacks and nightmares.
- Pre-screen: Identified a highly reactive trauma event (loss of service dog). Autonomic arousal observed during brief recounting.
- Intake: Detailed recounting of the trauma event ("Rocket Attack, 1971") with significant autonomic arousal.
- Treatment 1:
- Practice movies used to familiarize Carl with the visual formats.
- "Rocket Attack, 1971" addressed using RTM steps: multiple iterations of black and white dissociated viewing, associated colour reversal, and revised, safer outcome movies. SUDs reduced from 8 to 0.
- A second trauma ("Viet Cong Sapper") addressed similarly, reducing SUDs from 8 to 0. The treatment involved multiple iterations of black and white dissociated viewing, associated color reversal, and the creation of safer outcome narratives. The therapist noted specific changes in Carl's responses, such as a reduction in the perceived duration of the event.
- Follow-up: Significant reduction in PTSD symptoms maintained at 2, 6, 26, and 52 weeks post-treatment.
- Conclusions: The case study demonstrates RTM's potential as a highly effective, brief intervention for PTSD. Further research is warranted. The therapists' skills in rapport-building and calibration were highlighted as essential factors in achieving positive outcomes. The study's limitations include its small sample size and the reliance on self-reported data.
To read the full case study https://reprogrammingmind.com/how-to-cure-ptsd-four-times-in-5-hours/

What’s the Best Way to Write a Breakup Letter?

How Your Memories Affect Your Decision Making – Dr. Jordan Peterson

Common Mistakes People Make After a Breakup

How can I overcome the memories of my ex?
25 Empowering Movies to Overcome Heartbreak, Get Over a Breakup and Ignite Self-Discovery
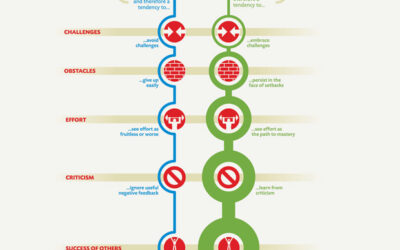
Minding Success: Navigating the Power of Dwecks Growth vs Fixed Mindset
Navigating Heartbreak: 6 Steps Women Who End Up Happier After A Breakup Do During The Healing Process

How to Heal and Open Your Heart After a Breakup

Habit Stacking Examples to Get Over a Breakup